Accuracy of freehand external ventricular drain placement in patients after a large decompressive hemicraniectomy
Authors
Cezar José Mizrahi¹, Iddo Paldor², Carlos Candanedo³, Semira Mollica¹, Eyal Itshayek⁴
- Department of Neurosurgery, Royal Melbourne Hospital, University of Melbourne, Melbourne, Victoria, Australia
- Department of Neurosurgery, Rambam Health Care Campus, Haifa, Israel
- Department of Neurosurgery, Hadassah-Hebrew University Medical Center, Jerusalem, Israel
- Department of Neurosurgery, Rabin Medical Center, Petah Tikva, Israel
Article Info
- Received: 17 July 2020
- Accepted: 6 September 2020
Keywords
Accuracy, Craniectomy, Decompressive craniectomy, External ventricular drain, Freehand
Abstract
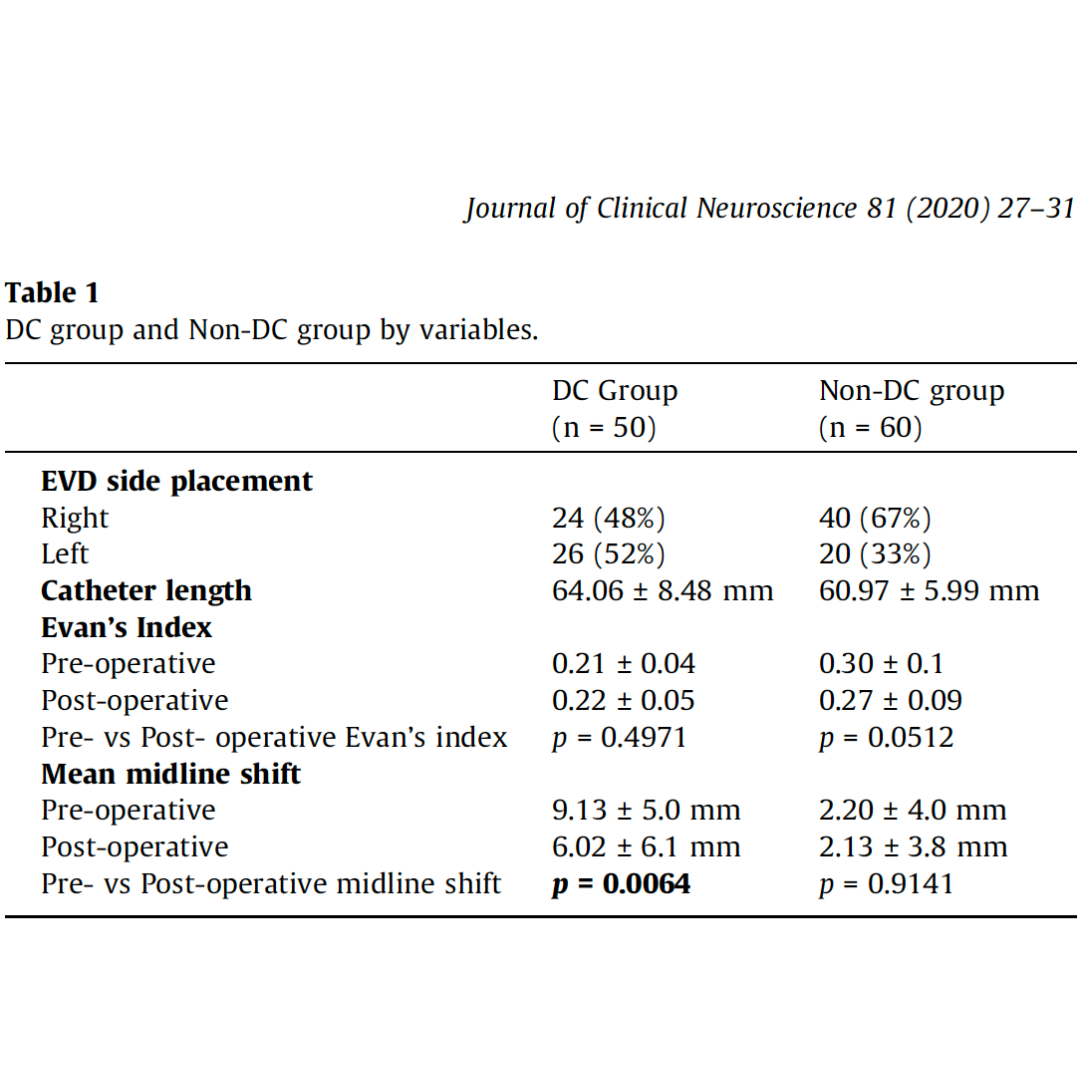
Our study aim is to evaluate the accuracy of freehand external ventricular drain (EVD) placement, without the use of adjuncts to placement, immediately following a large decompressive hemicraniectomy (DC). We performed a retrospective cohort analysis comparing patients who underwent freehand EVD placement immediately after a DC, to those who underwent freehand EVD placement without DC. Computed tomography (CT) studies were used to assess accuracy based on catheter tip location. Intracranial catheter length, pre- and post-operative Evan’s Index, and midline shift pre- and postoperatively were analysed as separate variables in each group. A previously described grading system was used to assess the accuracy of freehand EVD placement.
There were a total of 110 patients overall: DC group, n = 50; non-DC group, n = 60. There was a significant reduction from pre-operative midline shift to post-operative midline shift in the DC group (9.13 vs 6.02 mm; p = 0.0064). There was no significant difference in accuracy between the two groups (p = 0.8917), and similar rates of Grade 1 – i.e. optimal – catheter tip location (DC = 78% vs non-DC = 81%) were found. All analysed variables comparing both Grade 1 subgroups (pre- and postoperative Evan’s Index, and midline shift) showed significant differences between them. Mean catheter length in Grade 1 EVD placement showed a statistically significant difference between the DC and non-DC groups (63.78 vs 59.96 mm, respectively; p = 0.009).
An EVD, after DC for traumatic and non-traumatic intracranial pathologies, can be accurately placed by freehand.