CPA Epidermoid Cyst with Rare Anatomic Variant:
Anterior Inferior Cerebellar Artery Embedded in the Subarcuate Fossa: Operative Video and Technical Nuances
Carlos Candanedo¹, Sergey Spektor¹
¹Department of Neurosurgery, Hadassah-Hebrew University Medical Center, Jerusalem, Israel
Published in: Journal of Neurological Surgery Part B, 2019; 80 (Suppl S3): S323–S324.
Correspondence:
Carlos Candanedo, MD
Department of Neurosurgery, Hadassah-Hebrew University Medical Center
P.O. Box 12000, Jerusalem, Israel 91120
Email: ccandanedomd@hotmail.com
Keywords:
- Epidermoid cyst
- Trigeminal neuralgia
- Anterior inferior cerebellar artery (AICA)
- Subarcuate artery
- Operative video
Abstract
Intracranial epidermoid cysts are considered benign tumors with a good general prognosis; however, their radical removal, including the tumor capsule, is associated with significant morbidity, especially when the capsule is attached to neurovascular structures.
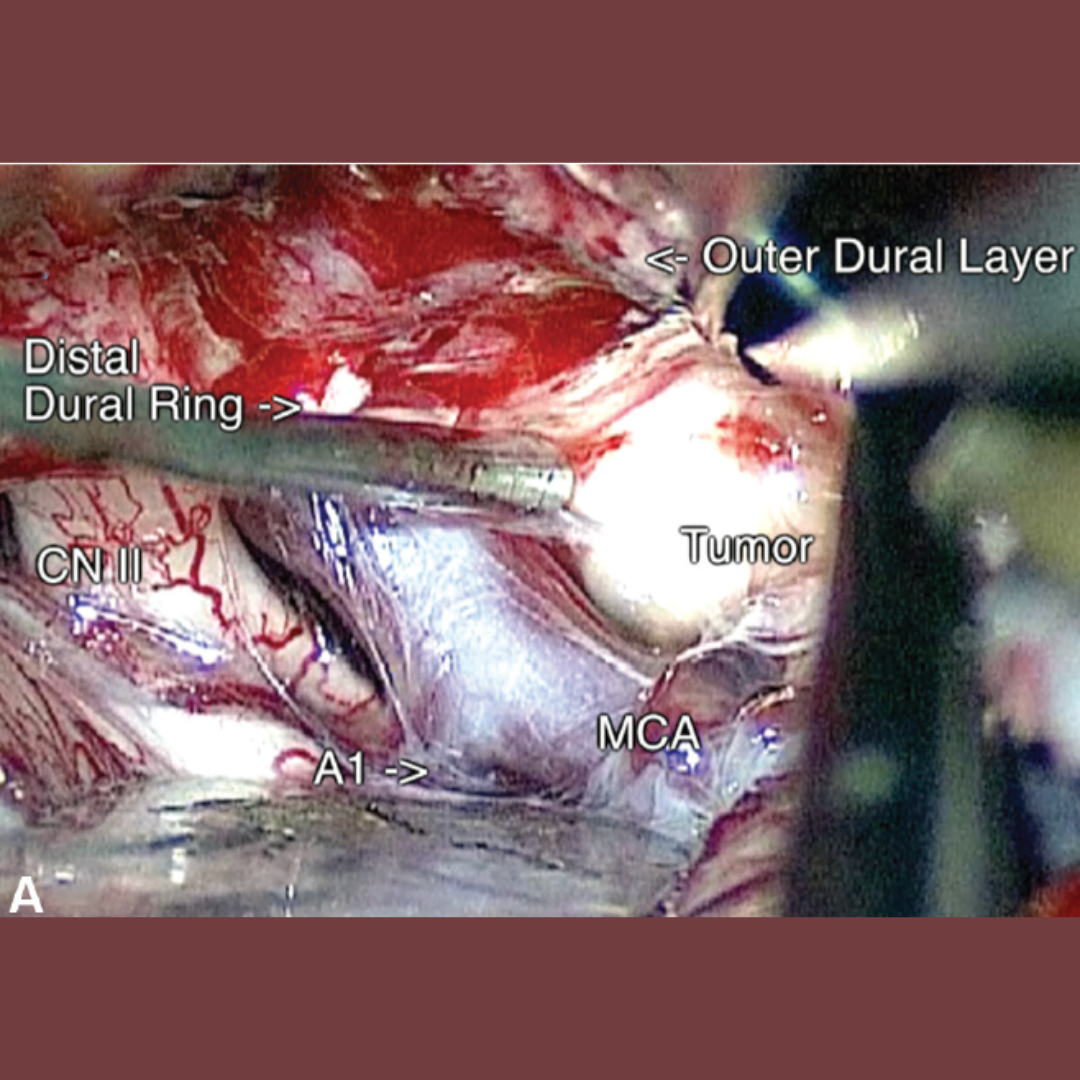
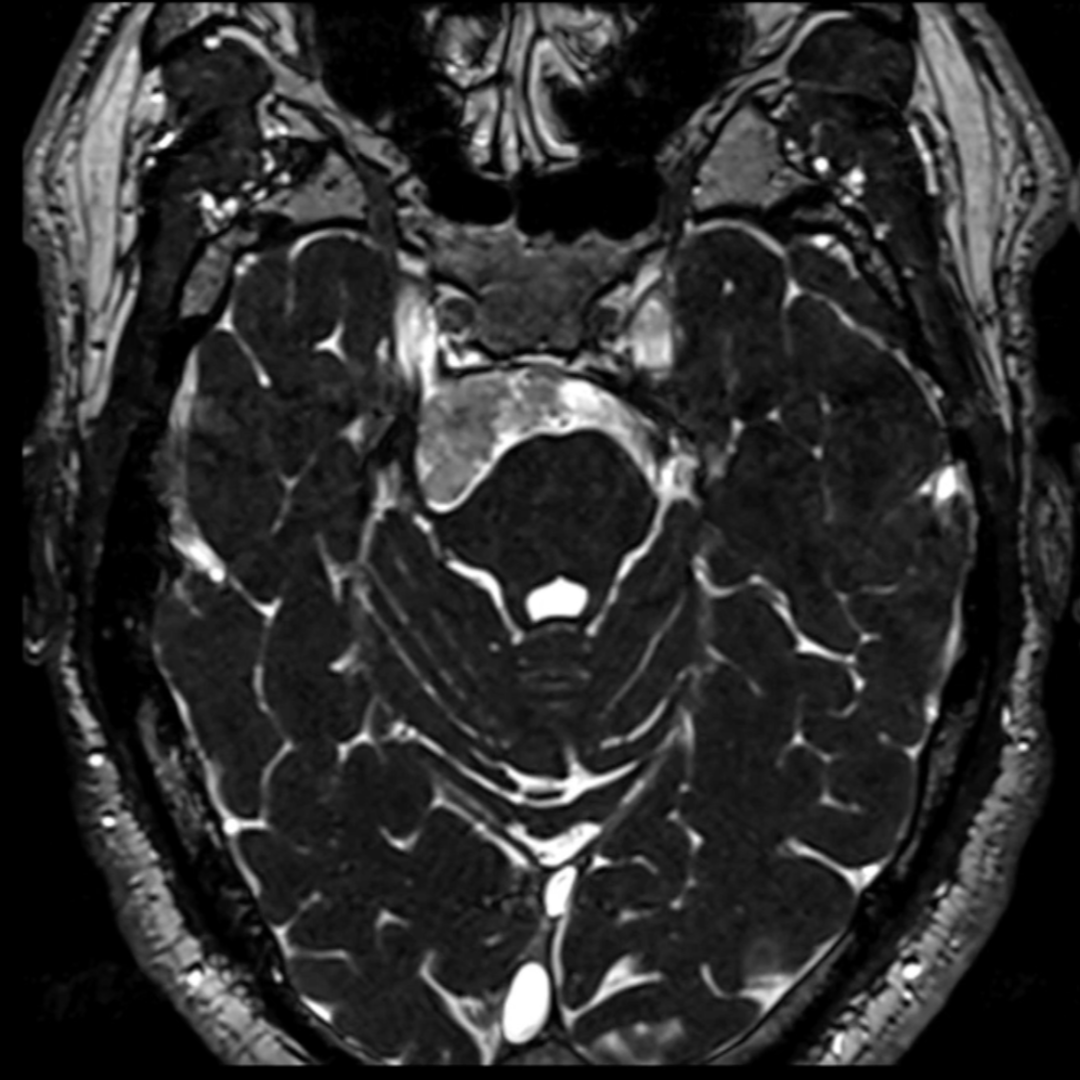
This report includes an operative video detailing the main steps and surgical nuances in the resection of a large right cerebellopontine angle (CPA) epidermoid cyst in a 42-year-old male patient presenting with intractable trigeminal neuralgia.
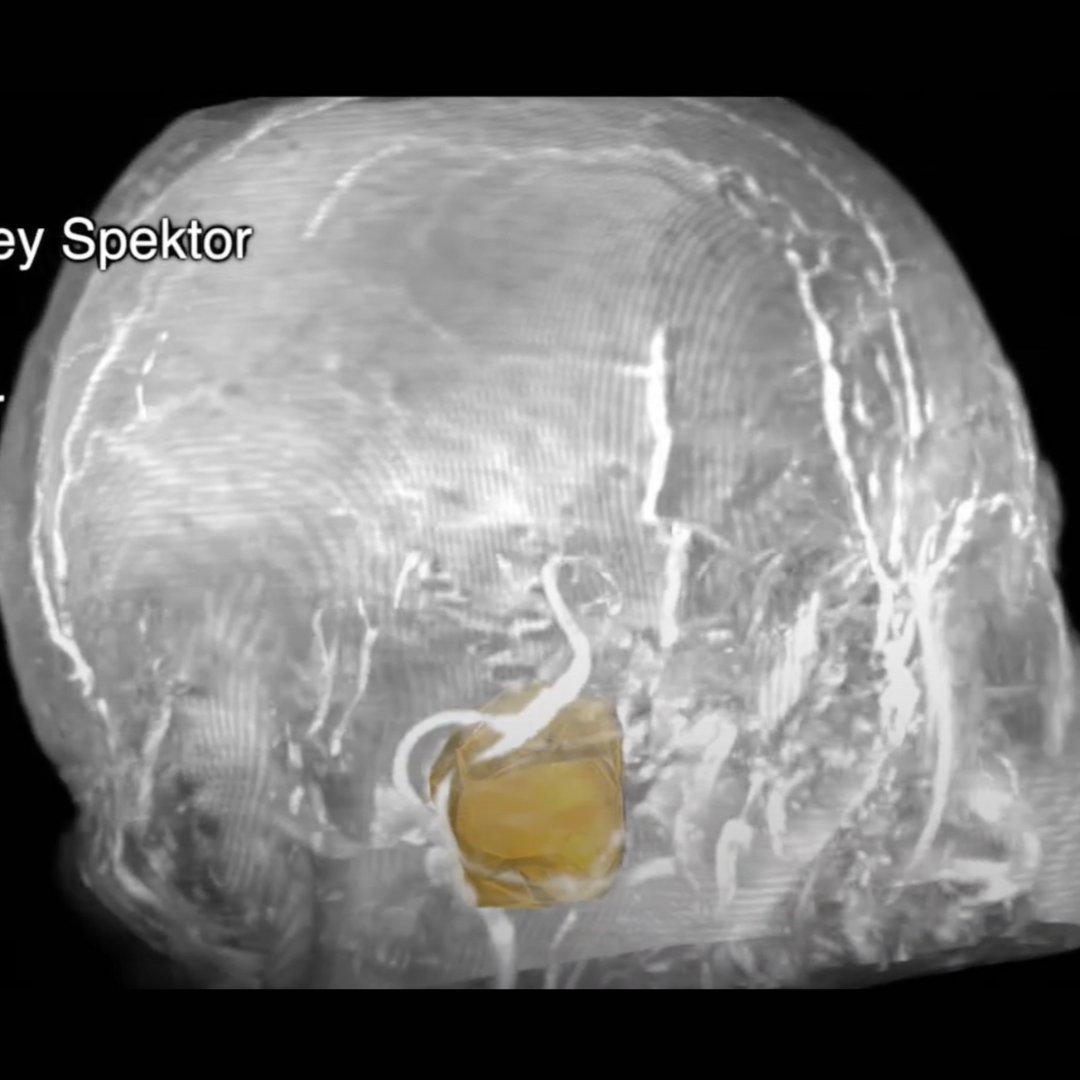
A craniectomy was performed to expose the transverse-sigmoid sinus junction. Before opening the dura, a mold for a polymethylmethacrylate (PMMA) bone flap was built to avoid potentially neurotoxic effects on the cerebellum. The video highlights the management of a rare anatomical variant of the anterior inferior cerebellar artery (AICA), whose loop was embedded in the dura covering the subarcuate fossa, where it gives off the subarcuate artery.
Near-total removal of the epidermoid cyst was achieved, leaving only a small remnant of the capsule adhering to the abducens nerve. Postoperatively, the patient’s trigeminal neuralgia was completely resolved, and medications were discontinued. The patient’s hearing was preserved at the preoperative level (Gardner–Robertson II), as confirmed by audiometry. Postoperative magnetic resonance imaging (MRI) showed no signs of residual tumor.
In this case, optimal surgical exposure of the CPA was not possible without addressing the rare anatomical anomaly of the AICA in the dura of the subarcuate fossa. This required coagulation and transection of the subarcuate artery and transposition of the AICA with the dural cuff. This manipulation enabled complete surgical removal of the epidermoid cyst and did not result in any neurological deficit.
The video can be accessed at: https://youtu.be/lLZqBHlu-uA.