Cavernous Sinus Epidermoid Cyst Removal through a No-Keyhole Pterional Craniotomy: Operative Video and Technical Nuances
Authors:
Carlos Candanedo¹, Samuel Moscovici¹, Sergey Spektor¹
¹Department of Neurosurgery, Hadassah-Hebrew University Medical Center, Jerusalem, Israel
Journal:
Journal of Neurological Surgery B
Address for Correspondence:
Carlos Candanedo, MD
Department of Neurosurgery
Hadassah-Hebrew University Medical Center
P.O. Box 12000, Jerusalem 91120, Israel
(e-mail: ccandanedomd@hotmail.com)
Keywords
- Anterior clinoidectomy
- Cavernous sinus
- Epidermoid cyst
- Oculomotor nerve
- Operative video
- Posterior petroclinoid ligament
- Pterional craniotomy
Abstract
Intracranial epidermoid cysts are considered benign tumors with good general prognosis. However, their radical removal may be associated with certain morbidity, especially when the capsule is attached to neurovascular structures. Epidermoid cysts located in the cavernous sinus are very rare.
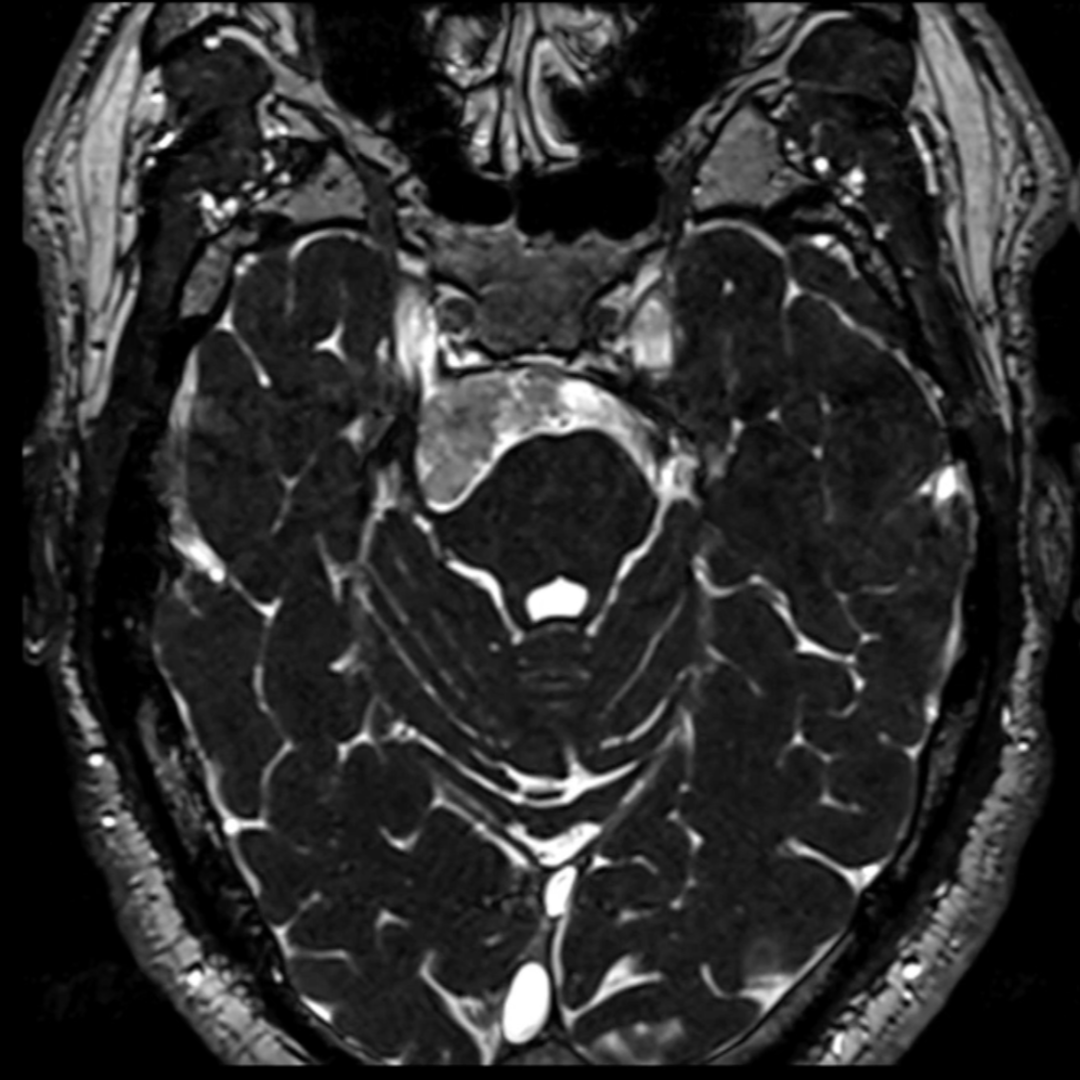
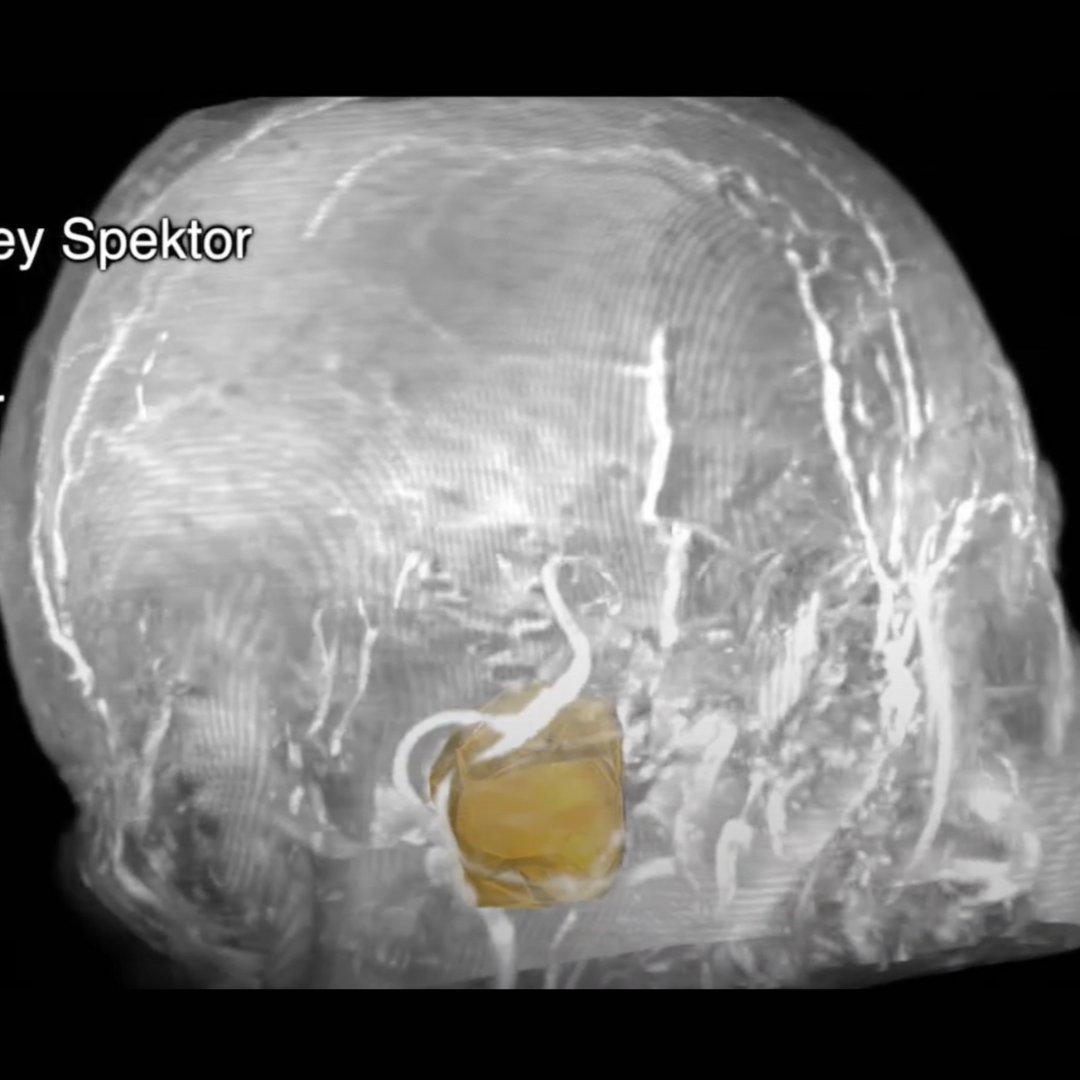
We present an operative video of a 22-year-old female patient, who suffered from a right-sided headache for 5 years. The video demonstrates the main steps and surgical nuances of resection of a right interdural cavernous sinus epidermoid cyst, measuring 22 × 19 × 21 mm (4.3 cc) (►Fig. 1A).
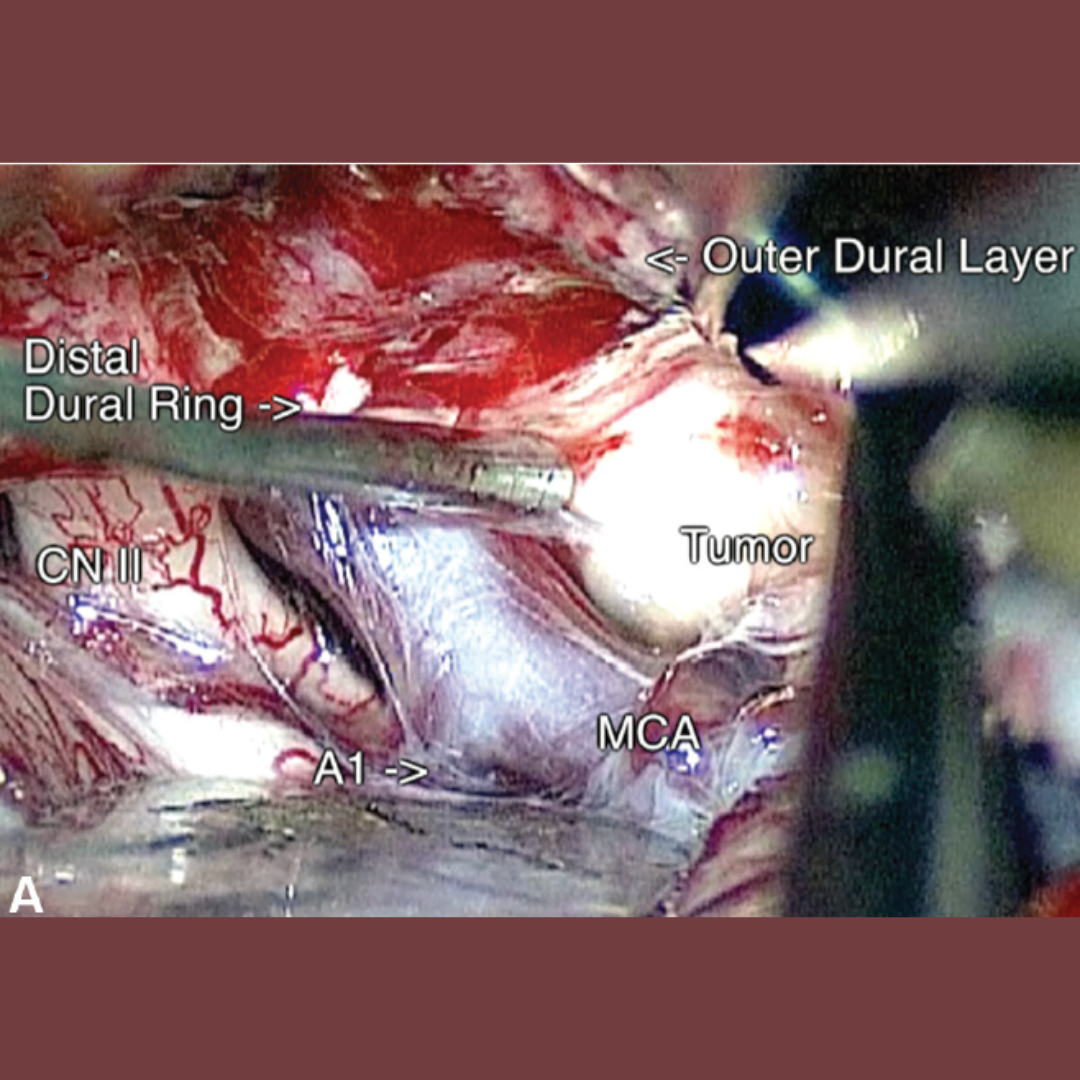
On initial physical examination, the patient had a right partial third nerve palsy (mild ptosis with minimal diplopia), without any other cranial nerve deficit. A right no-keyhole pterional craniotomy was performed, followed by extradural anterior clinoidectomy and peeling of the outer dural layer of the lateral wall of the cavernous sinus. The dura mater was also detached from the distal carotid dural ring, which was exposed by the clinoidectomy (►Fig. 2A).
This maneuver provided excellent exposure of the interdural epidermoid cyst, which severely compressed the oculomotor nerve against the posterior petroclinoid dural fold (►Fig. 2B). Gross total resection of the epidermoid cyst was achieved (►Fig. 1B and C).
The patient developed a transient worsening of the third nerve palsy, which recovered completely 3 months after the surgery. Postoperative magnetic resonance imaging revealed no signs of residual tumor.
The link to the video can be found at: https://youtu.be/pobhYb5ZNig.