Clival Meningioma Removal through a Suboccipital Retrosigmoid Approach: Operative Video and Technical Nuances
Carlos Candanedo¹, Samuel Moscovici¹, Sergey Spektor¹
¹ Department of Neurosurgery, Hadassah-Hebrew University Medical Center, Jerusalem, Israel
J Neurol Surg B 2021; 82(Suppl S1): S27–S28.
Address for correspondence:
Carlos Candanedo, MD,
Department of Neurosurgery,
Hadassah-Hebrew University Medical Center,
P.O. Box 12000, Jerusalem, Israel, 91120
(e-mail: ccandanedomd@hotmail.com)
Keywords
- Clival meningioma
- Retrosigmoid approach
- Foramen magnum
- Operative video
- Low cranial nerves
Abstract
Background
Clival meningiomas are challenging lesions that need to be managed according to the displacement of the adjacent structures. Lateral skull base approaches are required to achieve their radical removal; however, they are associated with significant morbidity, especially when the tumor involves the basilar artery, its perforators, brainstem, and lower cranial nerves.
Design
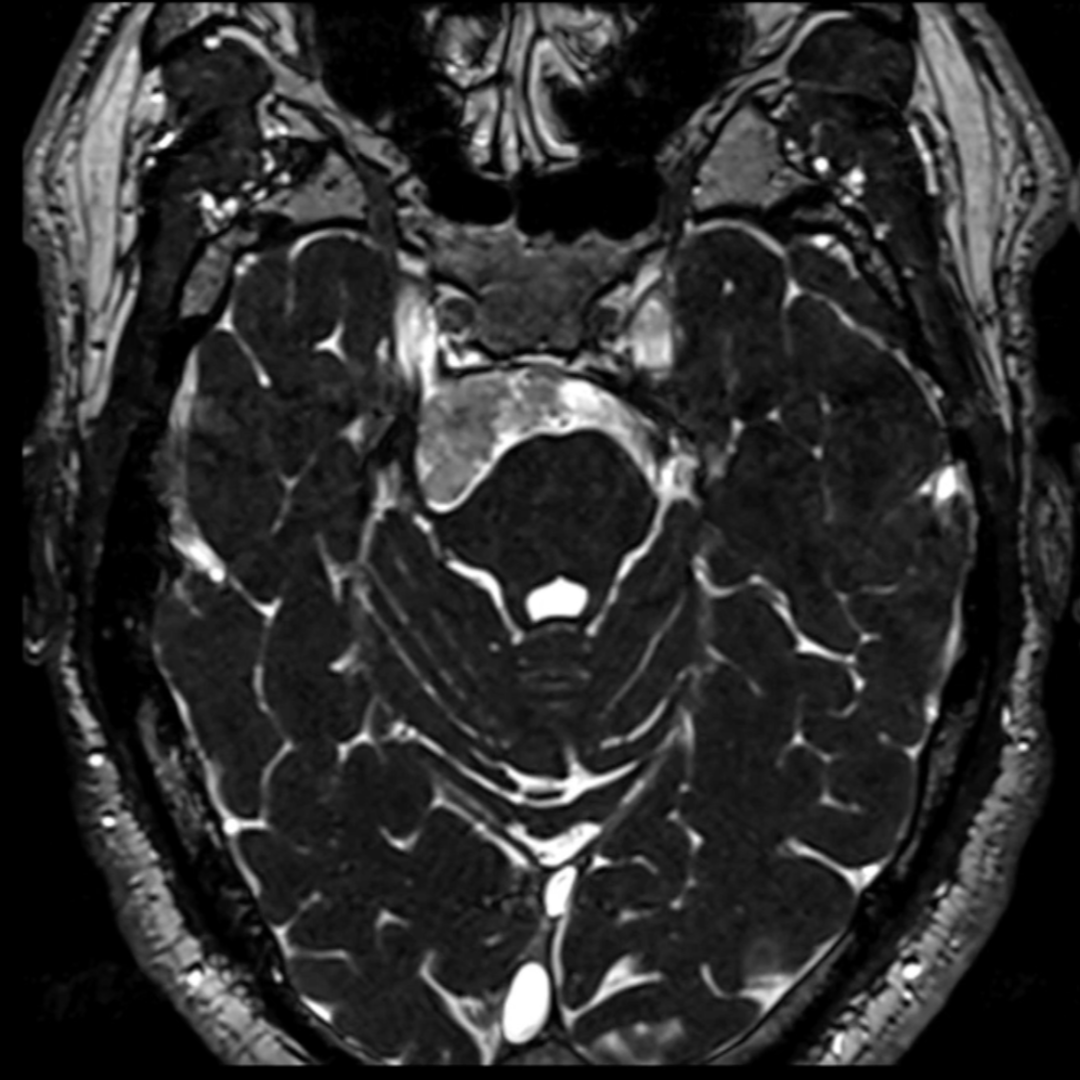
This is a case of a 79-year-old female patient, diagnosed with a large lower clival meningioma after experiencing headaches. A conservative treatment was initially offered, but serial MRI revealed an increase in the tumor’s size. Consequently, it was decided to remove the meningioma using a left suboccipital retrosigmoid approach.
Settings
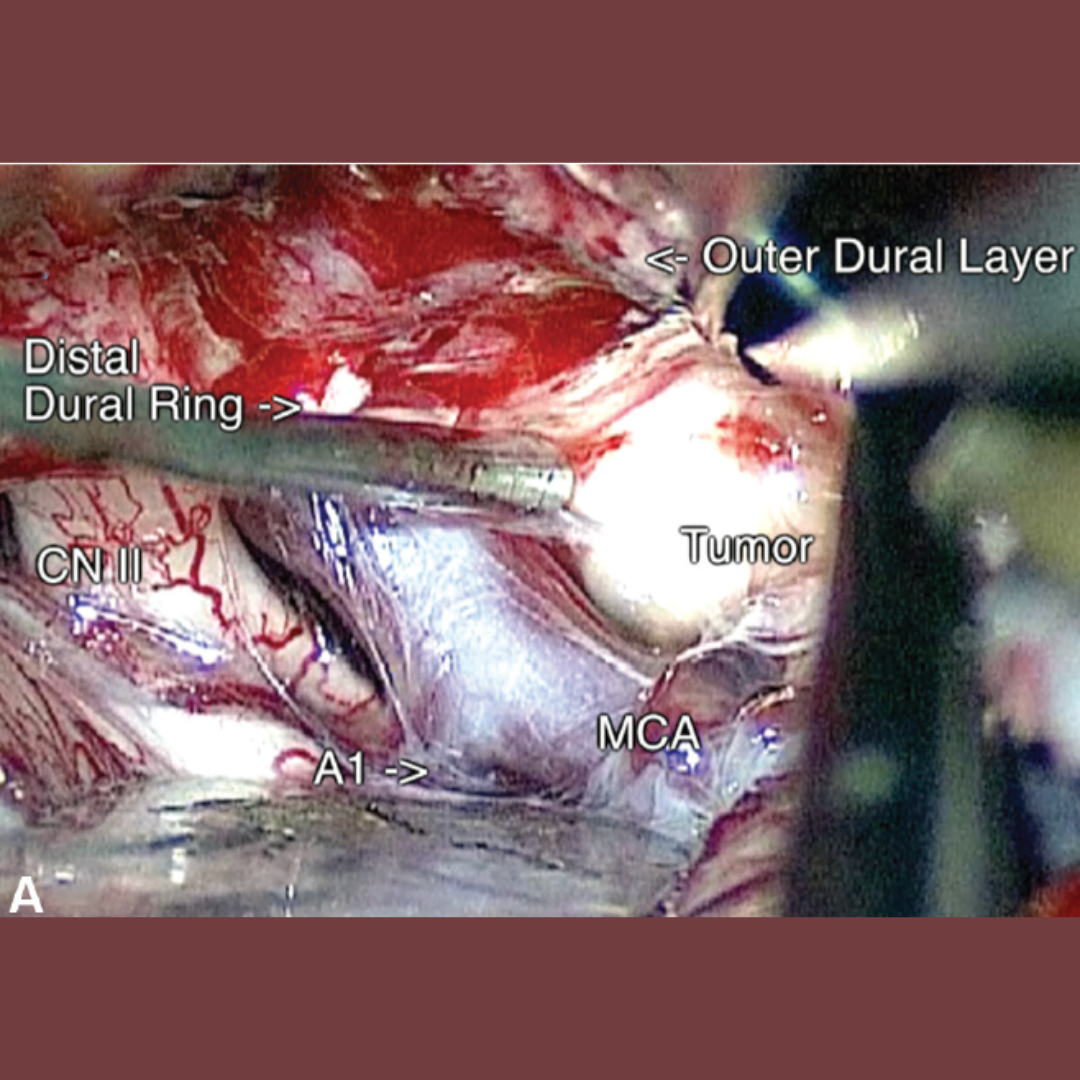
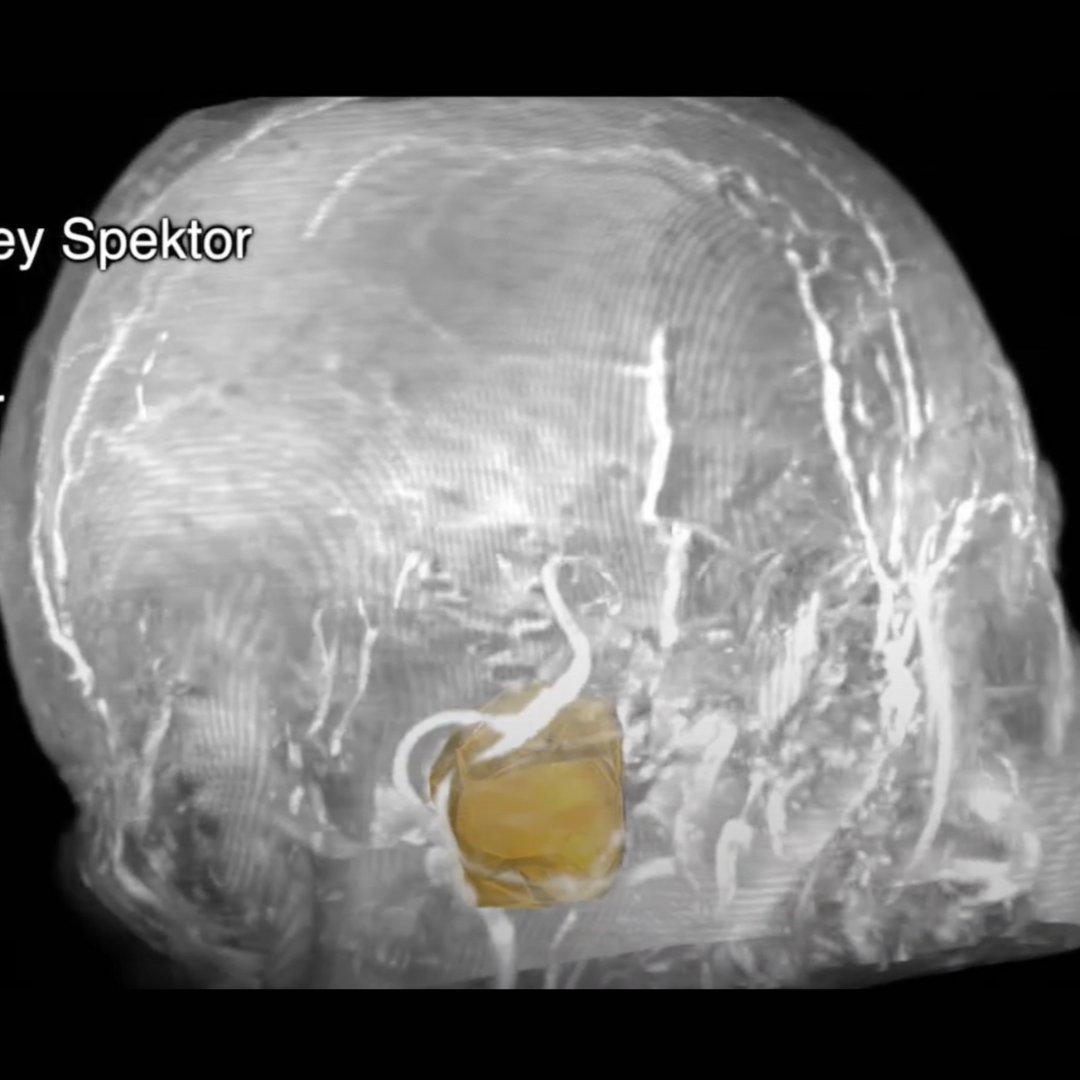
In a left three-quarter prone position, with neurophysiologic monitoring of the facial nerve, auditory brainstem response, lower cranial nerves, motor-evoked potentials, and somatosensory-evoked potentials, a left suboccipital retrosigmoid craniotomy with opening of the foramen magnum was performed. This approach provided sufficient lateral visualization of the tumor. The broad-based tumor, which was displacing the vertebral and basilar arteries, cranial nerves (7th–12th), and the brainstem, was exposed and removed.
Results
Near-total resection of the meningioma was achieved, leaving only a microscopic residual at the entry points of the lower cranial nerves, without complications. There was no neurological deficit post-surgery. Postoperative MRI revealed no signs of residual tumor.
Conclusion
In this case, the regular retrosigmoid approach, extended into the foramen magnum, was sufficient for the removal of this pure clival meningioma.
The link to the video can be found at:
https://youtu.be/3d6Uj4gjmDU